One of evolution’s cleverest tricks was
giving us a sense of shame. It’s a miserable feeling—low, humbling,
publicly discomfiting—but it’s supposed to be: if you do something lousy
you ought to feel something lousy, so you don’t do it again.
In theory, when so many of the strategies for beating the COVID-19 pandemic
depend on abiding by social distancing and other rules, shaming people
who don’t ought to be a powerful way to bring us back in line. But
increasingly, experts believe, the opposite is true. “The thinking has
been that the more you shame people the more they will obey,” says
Giovanni Travaglino, an assistant professor of social psychology at Kent
University. “But this turns out to be absolutely wrong.”
Last month, Travaglino and Chanki Moon, an assistant professor of psychology at Leeds Beckett University, published a paper in Frontiers in Psychology
that threw the ineffectiveness of shaming into relief. They assembled
nearly 1,900 people from the U.S., Italy and South Korea—choosing those
countries on the basis of their differing sense of the collective
culture, with the U.S. judged the most individualistic, South Korea the
most group-oriented and Italy in between. The subjects were asked to
rate how ashamed or guilty they’d feel if they contracted COVID-19. They
were also asked to rate how often they obey guidelines like social
distancing and how likely they’d be to tell friends, acquaintances and
health authorities if they tested positive. In all three countries, the
higher the level of shame and guilt people felt over falling ill, the
less likely they were to play it safe and to report their COVID-19 status.
In the U.S. and elsewhere, the antivaccine movement
has long been a threat to public health, and many pro-vaccine messages
have been designed to shame adherents. A December story in the U.K.’s
Metro featured the headline “People think anti-vaxxers are ‘stupid and
selfish.'” Attention-grabbing, maybe, but counterproductive. “It’s hard
to get people to act in a cooperative manner when you approach them that
way,” says Travaglino. “It’s associated with subordination to
authority, and people don’t like that.”
A new
TIME/Harris Poll survey similarly suggests individual authority figures
aren’t very effective at convincing vaccine skeptics.
Of U.S. adults who had recently been vaccinated,
only 32% said they were influenced by a local official reaching out
directly via email, phone or mail. Much more effective, it seems, are
appeals to people’s individual needs and desires. Some 52% of those
polled said they got the vaccine because they wanted to travel, for
example. The people around us also play a major role, with 56% of
respondents saying they got vaccinated after a friend or family member
did, and 59% saying they were influenced merely by having a conversation
with such a closely connected person. And despite our ostensible
mistrust in the media, 63% said they were influenced by news reports
about people who had already been vaccinated.
Indeed, past research shows value in appealing to us through personal stories. In a 2015 study published in the PNAS,
volunteers took a survey on their attitudes about vaccines and were
then divided into three groups, each given one of three things to read:
material showing that autism and vaccines are not related; a paragraph
of a mother describing her child’s bout with measles; and material on an
unrelated science topic. When the subjects took the vaccine survey
again, all were more pro-vaccine than before, but the ones who read the
mother’s account were dramatically more so, with an increase five times
as great as that of the group that had read the material on autism and
six times that of the control group.
Personal accounts can have a negative impact too. A new study published in PLOS ONE,
by researchers from the University of Illinois and the Annenberg Public
Policy Center, found that subjects who saw a video clip of Dr. Anthony
Fauci talking about the safety and effectiveness of the measles vaccine
came away from it more favorably disposed to vaccination overall. But
the positive effect was diminished when they saw another video clip
first, of a mother describing the severe rash one of her children
developed after receiving the vaccine. The solution, the paper
concluded, is not for the media to censor such accounts but to precede
them with real-world data on the minimal risks and the considerable
benefits of vaccines.
When the polio vaccine was declared safe and effective, the news was met with jubilant celebration. Church bells rang across the nation, and factories blew their whistles. “Polio routed!” newspaper headlines exclaimed. “An historic victory,” “monumental,” “sensational,” newscasters declared. People erupted with joy across the United States. Some danced in the streets; others wept. Kids were sent home from school to celebrate.
Your guide to life on a warming planet
Discover Atlantic Planet, a new section devoted to climate change and the ways it will reshape our world
One
might have expected the initial approval of the coronavirus vaccines to
spark similar jubilation—especially after a brutal pandemic year. But
that didn’t happen. Instead, the steady drumbeat of good news about the
vaccines has been met with a chorus of relentless pessimism.
The
problem is not that the good news isn’t being reported, or that we
should throw caution to the wind just yet. It’s that neither the
reporting nor the public-health messaging has reflected the truly
amazing reality of these vaccines. There is nothing wrong with realism
and caution, but effective communication requires a sense of
proportion—distinguishing between due alarm and alarmism; warranted,
measured caution and doombait;
worst-case scenarios and claims of impending catastrophe. We need to be
able to celebrate profoundly positive news while noting the work that
still lies ahead. However, instead of balanced optimism since the launch
of the vaccines, the public has been offered a lot of misguided
fretting over new virus variants, subjected to misleading debates about the inferiority of certain vaccines, and presented with long lists of things vaccinated people still cannot do, while media outlets wonder whether the pandemic will ever end.
After nine months of social distancing, masking and quarantining, many people are experiencing pandemic fatigue.
Newswise
— The sharp rise in COVID-19 cases throughout Pennsylvania and across
the United States makes continued vigilance with established safety
efforts essential to helping slow the virus’s spread. Yet after nine
months of social distancing, masking and quarantining, many are
experiencing pandemic fatigue. Whether it manifests as anxiety,
exhaustion or defiance, it’s important to recognize and address it for
the sake of our physical and emotional health.
A long and uncertain pandemic
Health
care providers on the frontlines of the COVID battle have seen how
approaches to treatment and prevention have evolved, sometimes seemingly
overnight, often resulting in a sense of uncertainty, anxiety or even
doubt with the public.
One
of the most significant evolutions he has witnessed — one that may have
played a role in some people’s continued unwillingness to mask properly
— is guidance on face coverings for the general public.
“At
first, we were told that only health care workers needed to wear a
mask,” Nunez said. “But since those early days, there's been a lot of
evidence overall that wearing masks may definitely slow the spread of
the virus and help people from transmitting it to others, especially if
they’re asymptomatic.”
Another theory from early in the pandemic
was that the warmer weather over the summer would potentially halt the
virus, as it does with other seasonal respiratory diseases. “Super
spreader events in the form of outdoor gatherings showed that this
unfortunately wasn’t the case for COVID,” Nunez said.
Nunez
advises that anyone considering in-person activities like dining out or
shopping make sure that everyone in the establishment is abiding by the
rules. “Are they wearing masks, covering the whole face, sitting six
feet apart?” he asked, adding that even with these measures, “there is
no absolute decreased risk.” He prefers creative solutions to social
gatherings. “Most of my inspiration has come from the internal medicine
residents. They've been able to continue their game nights — virtually.”
Minding your mental health
The
relentless pace of the pandemic and the resulting social distancing
restrictions have been exhausting and stressful, explains Dr. Julie Graziane,
a psychiatrist at the Milton S. Hershey Medical Center. “But there are
things that we can do to help mitigate a lot of those stressful
emotions,” she said.
Graziane suggests an emotional reframing of
quarantines and social distancing restrictions. “Don’t think of them as
things we’re being forced to follow, but rather as actions we're freely
choosing to do to help others,” she said. “We shift it into an
altruistic action as we do these things to help our loved one, our
neighbor, even the stranger in the community that we care about.”
The colder weather and fewer hours of daylight can add to the emotional burden of that COVID causes.
“We’ve
been watchful with mental health as individuals experience significant
emotional stress during the pandemic,” Graziane said. “And we’re
especially concerned as we head into the winter months that play a role
in some people’s depression.”
One significant stressor from COVID
that Graziane points to is the disruption to routines, such as getting
the kids on the bus in the mornings or driving to work. She recommends
establishing new routines.
“Have a regular awake time or regular
sleep time, and regular meal times,” Graziane said. “Then take some time
during the day to check in with yourself, how you're feeling about the
day, the situation. Incorporating healthy activities like exercise and
mindfulness, and then pleasurable activities.”
Reflecting on what
was important to them and provided meaning to their lives prior to the
pandemic can help people find strength and purpose as quarantines
continue, Graziane said. “And don’t be afraid to reach out for help. If
you feel like you're struggling with getting through this, talk to
someone such as a loved one, a physician, a counselor or a friend.”
Nunez
stresses that we take the time to check in with others. “Maybe someone
you know is struggling and just because you don’t ask, they don’t
mention it,” he said. “We’re all going through this. We are not alone.”
Hopeful while remaining vigilant
While
recent news that an effective vaccine is expected to come to market
soon points to an eventual end to the pandemic and its social
restrictions, both Graziane and Nunez stress that the general population
is still perhaps months away from being able to receive the two-part
vaccination.
“For now, we must remain ever vigilant,” Graziane said.
“I
think what’s important this holiday season is remembering that we’re
trying to stay healthy and we’re also really trying to keep others
healthy,” said Nunez, “especially our patients who are vulnerable and at
risk for severe complications of the disease.”
The Medical Minute is
a weekly health news feature produced by Penn State Health. Articles
feature the expertise of faculty, physicians and staff, and are designed
to offer timely, relevant health information of interest to a broad
audience.
Give a shoutout to CDC on social or copy the text below to attribute.
Since the early days of the pandemic, attention has focused on
producing a vaccine for COVID-19. With one, it’s hoped it will be able
to suppress the virus without relying purely on economically challenging
control measures. Without one, the world will probably have to live
with COVID-19 as an endemic disease. It’s unlikely the coronavirus will naturally burn itself out.
With so much at stake, it’s not surprising that COVID-19 vaccines
have become both a public and political obsession. The good news is that
making one is possible:
the virus has the right characteristics to be fended off with a
vaccine, and the economic incentive exists to get one (or indeed
several) developed.
But we need to be patient. Creating a new medicine requires a large amount of thought and scrutiny
to make sure what’s produced is safe and effective. Researchers must be
careful not to allow the pressure and allure of creating a vaccine
quickly to undermine the integrity of their work. The upshot may be that
we don’t have a highly effective vaccine against COVID-19 for some
time.
Here, authors from across The Conversation outline what we know so
far. Drawing upon their expertise, they explain how a COVID-19 vaccine
will work, the progress a leading vaccine (developed by the University
of Oxford with AstraZeneca) is making, and what challenges there will be
to manufacturing and rolling a vaccine out when ready.
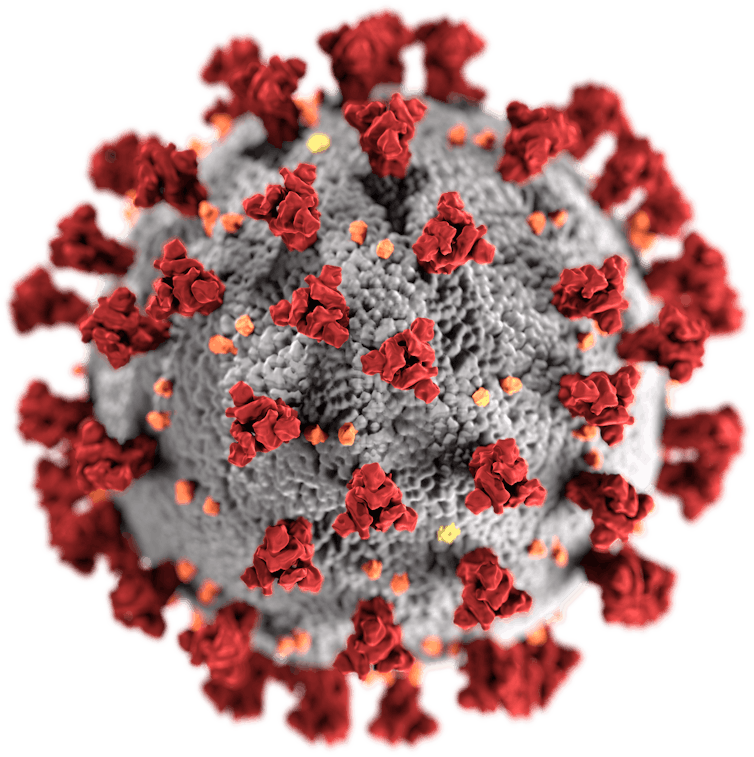
Although the way the body interacts with SARS-CoV-2 isn’t fully
understood, there’s one particular part of the virus that’s thought to
trigger an immune response – the spike protein, which sticks up on the
virus’s surface. Therefore, the two leading COVID-19 vaccines both focus
on getting the body to produce these key spike proteins, to train the immune system to recognise them and destroy any viral particles that exhibit them in the future.
SARS-CoV-2, with its spike proteins shown in red.US Centers for Disease Control and Prevention/Wikimedia Commons
The pros and cons of different designs
The leading vaccines both work by delivering a piece of the
coronavirus’s genetic material into cells, which instructs the cell to
make copies of the spike protein. As Suresh Mahalingam and Adam Taylor explain,
one (Moderna’s) makes the delivery using a molecule called messenger
RNA, the other (AstraZeneca’s) using a harmless adenovirus. These
cutting-edge vaccine designs have their pros and cons, as do traditional
methods.
Boosters may be needed
The strongest immune responses,
says Sarah Pitt, come from vaccines that contain a live version of what
they’re trying to protect against. Because there’s so much we don’t
know about SARS-CoV-2, putting a live version of the virus into a
vaccine can be risky. Safer methods – such as getting the body to make
just the virus’s spike proteins, or delivering a dead version of the
virus – will lead to a weaker response that fades over time. But
boosters can top this up.
if boosters are required, manufacturing sufficient doses and delivering them will become an even greater challenge.SiphiIwe Sibeko/EPA
What governs how we respond to vaccines?
A vaccine’s design isn’t the only factor that determines how strong our
immune response is. As Menno van Zelm and Paul Gill show, there are four other variables
that make each person’s response to a vaccine unique: their age, their
genes, lifestyle factors and what previous infections they have been
exposed to. It may be that not everyone gets long-lasting immunity from a
vaccine.
Why vaccines provide strong immunity
If well-designed, a vaccine can provide better immunity
than natural infection, says Maitreyi Shivkumar. This is because
vaccines can focus the immune system on targeting recognisable parts of
the pathogen (for example the spike protein), can kickstart a stronger
response using ingredients called adjuvants, and can be delivered to key
parts of the body where an immune response is needed most. For
COVID-19, this could be the nose.
Nasally delivered vaccines are already in use for some diseases, such as flu.Douglas Jordan, MA/CDC
How to use a vaccine when it’s available
Scientists think between 50% and 70% of people need to be resistant to
the coronavirus to stop it spreading. Using a vaccine to rapidly make
that many people immune might be difficult, says Adam Kleczkowski.
Vaccines are rarely 100% effective, and hesitancy and potential side
effects may make a quick, mass roll-out unrealistic. A better strategy might be to target people most at risk together with those likely to infect many others.
How is the Oxford vaccine being developed, tested and approved?
The many steps of vaccine development
Vaccine development is quicker now than it ever has been, explain
Samantha Vanderslott, Andrew Pollard and Tonia Thomas. Researchers can
use knowledge from previous vaccines, and in an outbreak more resources
are made available. Nevertheless, it’s still a lengthy process,
involving research on the virus, testing in animals and clinical trials
in humans. Once approved, millions of doses then need to be produced.
Phase 1 and phase 2 trials are successful
After showing promise in animals, the University of Oxford’s vaccine
moved onto human testing – known as clinical trials, which are split
into three phases. Here, Rebecca Ashfield outlines the joint phase 1 and
2 trial that the vaccine passed through to check that it was safe and elicited an immune response, and explains how the vaccine actually uses a separate virus – a chimpanzee adenovirus – to deliver its content into cells.
Production of the Oxford/AstraZeneca
vaccine in Latin America is taking place in Argentina; part of the
phase 3 trial is being run in Brazil.EPA-EFE
How the phase 3 trial works
Earlier
trial phases showed that the vaccine stimulated the immune system, as
expected. But the million-dollar question is whether this actually
protects against COVID-19. Finding out means giving the vaccine to thousands of people
who might be exposed to the coronavirus and seeing whether they get
sick. As Ashfield and Pedro Folegatti show, this requires running
vaccination programmes in countries across the world.
Testing was paused – and that’s OK
In September, the phase 3 trial of the Oxford vaccine was paused after a
patient fell ill with a possible adverse reaction. Understandably this
caused dismay, but it shouldn’t have, says Simon Kolstoe. Pauses like this are common,
as independent moderators are needed to assess exactly what has
happened. Often illnesses in trials are unrelated to what’s being
tested. But even if they are, that’s exactly what we want these tests to
show.
In the US arm of the trial, one-third of participants are receiving a saline injection as a control.DonyaHHI/Shutterstock
But vaccine makers need to be more open
AstraZeneca didn’t publicly reveal what caused the pause but did share
this information with investors. This, says Duncan Matthews, was an
example of an attempt to apply old methods of operating to a new situation.
Why we need to know what’s in placebos
A key part of clinical trials are placebos – alternative or inactive
treatments that are given to participants for comparison. But a key problem,
Jeremy Howick explains, is that some vaccine trials don’t reveal what
their placebos contain. Without knowing what benchmark is being used,
it’s then difficult for outsiders to understand the relative effect (and
side effects) the vaccine has.
How will the vaccine be made and rolled out?
Preparing enough for the whole world
Universal demand for a COVID-19 vaccine means production bottlenecks
are a risk. For the Oxford vaccine, production involves growing key
components in human embryonic kidney cells, before creating the actual
vaccine and then purifying and then concentrating it. Running this
process at industrial scale, say Qasim Rafiq and Martina Micheletti, is
one of the biggest challenges AstraZeneca faces.
AstraZeneca and its partners are aiming to manufacture 2 billion doses of its vaccine by the end of 2021.RGtimeline/Shutterstock
Tobacco – an unexpected ally?
Vaccines
contain organic products, which traditionally have been grown using
cell cultures in containers called bioreactors. Recently plants have
been adapted to function as bioreactors too, which could help production
be massively increased. Tobacco may be especially useful:
it grows quickly, is farmed all over the world, is leafy and easily
modifiable. The tech hasn’t been approved for mass producing medicines –
but demand may change that.
Keeping vaccines cool will be crucial
Because COVID-19 vaccines will contain biological material, they’ll need to be kept cold
right up until they’re delivered, explains Anna Nagurney. Fail to keep
them cool and they’ll become ineffective. Refrigeration will therefore
be a major challenge in any roll-out campaign; an estimated 25% of
vaccines are spoiled by the time they reach their destination. A potential solution could be to encase their heat-sensitive parts in silica.
Cold storage facilities will be needed to store vaccines, while refrigerated trucks and planes will be needed to move them.Tony Karumba/AFP via Getty Images
‘Vaccine nationalism’ threatens universal access
Some governments are signing agreements with manufacturers
to supply them with vaccines ahead of other countries. Poorer nations
risk being left empty handed – putting people at risk and preventing any
attempt to coordinate suppressing the coronavirus worldwide. It’s also
unclear how access is being priced in these deals.
How to counter vaccine nationalism
India can play a key role in avoiding this “richest-takes-all” scenario, says Rory Horner. It’s traditionally been a major supplier of medicines
to the global south, and has the capacity to create more vaccines for
COVID-19 than any other country in the world. India’s Serum Institute
has signed up to make 400 million doses of the Oxford vaccine this year,
but with a population of 1.35 billion, how many will go abroad isn’t
yet clear.
India’s track record in producing vaccines and key medical ingredients has led to it being labelled the ‘pharmacy of the world’.Shutterstock/ManoejPaateel
Who will get the coronavirus vaccine first?
We need to plan now, say Laurence Roope and Philip Clarke. Governments
have big decisions to make. The pandemic is akin to a war situation, so
there’s an argument these vital goods should be rationed and banned from
private sale. Authorities also need to decide who should be prioritised: those most vulnerable, people most likely to spread the virus, or those who can kickstart the economy by returning to work.
How do you counter resistance and scepticism?
Public resistance is a sizeable problem – but nothing new
Not all hesitancy is the same, says Annamaria Carusi.
As well as the hardcore anti-vaxxers, plenty may resist COVID-19
vaccines on safety or animal welfare grounds. Indeed, while anti-vaxxers
attract a lot of attention, their influence on vaccination rates is often overstated, argues Samantha Vanderslott. In fact, desire for a vaccine is so widespread and strong that anti-vaxxer positions may be harder to defend right now.
Resistance to a COVID-19 vaccine has been well-documented – but there is also overwhelming anticipation.EPA-EFE
The far right is exploiting the pandemic
A recent report from the United Nations Security Council warned that
extreme right-wing groups in the US are using the pandemic to
“radicalise, recruit, and inspire plots and attacks”. Blyth Crawford
gives a run-down of the major groups
at work in America – what their aims are, the methods they’re using to
reach people, and the key pieces of misinformation that they’re
peddling.
How to build trust in vaccines
The usual strategy is to double down on positive messaging. But a better strategy,
Mark Honigsbaum argues, would be to acknowledge that there’s a lot we
don’t know about how some vaccines work, but that the benefits of taking
vaccines far outweigh the risks. A further step could be to make sure
that manufacturers are liable should vaccine recipients suffer negative effects. Often manufacturers are exempt.
Looking ahead
The future is full of possibility. COVID-19, Sars, Mers and the
common cold are all caused by coronaviruses, and scientists are
considering whether it’s possible to create a vaccine that could offer protection against them all
– and perhaps even against an as yet unknown coronavirus we’re yet to
encounter. Admittedly, having a vaccine that can do this seems unlikely
in the near future.
We shouldn’t get ahead of ourselves, though, says Sarah Pitt. No
vaccine has yet completed its safety trials, and we can’t yet be sure
that any vaccine will permanently prevent people from catching COVID-19.
We need to prepare ourselves for the very real possibility that a COVID-19 vaccine only reduces the severity of symptoms or provides temporary protection.
The
coronavirus outbreak is causing confusion and panic, and misinformation
is rife. For crystal clear explanations on everything you need to know
about the pandemic, The Conversation is a global network drawing upon
over 70,000 experts to provide evidence-based advice on everything from
facemasks to hand washing. If you want to support our brand of
independent, not-for-profit journalism, please consider a donation.
This fall, children and adults should receive a flu shot to prevent widespread illness, as cases of COVID-19 and the seasonal flu are expected to rise, potential at the same time, says Loyola University Medical Center Chief Medical
Officer Kevin Smith, MD. The flu and COVID-19 also share many of the
same symptoms.
Newswise
— MAYWOOD, IL – This fall, children and adults should receive a flu
shot to prevent widespread illness, as cases of COVID-19 and the
seasonal flu are expected to rise, potentially at the same time, says
Loyola University Medical Center Chief Medical Officer Kevin Smith, MD.
The flu and COVID-19 also share many of the same symptoms.
It typically takes two weeks to develop immunity following a flu shot.
“The
flu vaccine is especially important for older adults, and anyone with a
chronic condition that makes them more vulnerable to severe flu or
COVID-19 symptoms and complications,” says Dr. Smith. “It is possible to
contract the flu and COVID-19 at the same time. There’s also a real
concern that flu and COVID-19 cases may simultaneously spike in the
U.S., which could seriously impact the health care system’s ability to
optimally care for all patients.”
The Centers for Disease Control
& Prevention recommends flu shots for anyone older than six months
old with “rare exceptions.” The flu season typically runs from October
through March. Flu shots are widely available and covered by insurance.
Flu vs. COVID-19 symptoms
The
flu and COVID-19 share many of the same symptoms, “and it can be really
difficult to distinguish between the two,” says Dr. Smith; however,
testing can provide a definitive diagnosis. Both COVID-19 and the flu
can cause:
Fevers
Cough
Difficulty breathing
Fatigue
Muscle aches
Sore throat
Headache
New loss of taste or smell
Sore throat
Congestion or runny nose
Runny or stuffy nose
Gastrointestinal issues, including vomiting and diarrhea (less often)
How to stay healthy this fall In addition to getting a flu shot, Dr. Smith recommends that everyone continue to adhere to CDC COVID-19 safety guidelines to prevent illness this fall and winter. The recommendations include:
Wearing a mask
Social distancing
Washing hands frequently
Covering your mouth when coughing or sneezing
Staying home if you are not feeling well
Monitoring your symptoms
When should you call the doctor?
“If
you have symptoms of COVID-19 or the flu, you should contact your
doctor or a health care provider,” says Dr. Smith. Loyola Medicine
offers both in-person and telehealth (video) care.
“It’s also
important that you monitor your symptoms and seek immediate care if you
or a loved one is having difficulty breathing, no longer eating or
drinking, and/or continues to have a high fever, especially one that
lasts several days or more."
To schedule an appointment with a Loyola Medicine physician, visit loyolamedicine.org or call 888-584-7888.
About Loyola MedicineLoyola
Medicine, a member of Trinity Health, is a nationally ranked academic,
quaternary care system based in Chicago's western suburbs. The
three-hospital system includes Loyola University Medical Center,
Gottlieb Memorial Hospital and MacNeal Hospital, as well as convenient
locations offering primary care, specialty care and immediate care
services from more than 1,800 physicians throughout Cook, Will and
DuPage counties. Loyola is a 547-licensed-bed hospital in Maywood that
includes the William G. & Mary A. Ryan Center for Heart &
Vascular Medicine, the Cardinal Bernardin Cancer Center, a Level 1
trauma center, Illinois's largest burn center, a certified comprehensive
stroke center and a children’s hospital. Loyola also trains the next
generation of caregivers through its academic affiliation with Loyola
University Chicago’s Stritch School of Medicine and Marcella Niehoff
School of Nursing. Gottlieb is a 247-licensed-bed community hospital in
Melrose Park with the newly renovated Judd A. Weinberg Emergency
Department, an adult day care program, the Loyola Center for Metabolic
Surgery and Bariatric Care and the Loyola Cancer Care & Research
facility at the Marjorie G. Weinberg Cancer Center. MacNeal is a
374-licensed-bed teaching hospital in Berwyn with advanced medical,
surgical and psychiatric services, acute rehabilitation, an inpatient
skilled nursing facility and a 68-bed behavioral health program and
community clinics. Loyola Medical Group, a team of primary and specialty
care physicians, offers care at over 15 Chicago-area locations. For
more information, visit loyolamedicine.org. You can also follow Loyola Medicine on LinkedIn,Facebook or Twitter.
About Trinity Health Trinity
Health is one of the largest multi-institutional Catholic health care
delivery systems in the nation, serving diverse communities that include
more than 30 million people across 22 states. Trinity Health includes
92 hospitals, as well as 106 continuing care locations that include PACE
programs, senior living facilities, and home care and hospice services.
Its continuing care programs provide nearly 2.5 million visits
annually. Based in Livonia, Mich., and with annual operating revenues of
$19.3 billion and assets of $27 billion, the organization returns $1.2
billion to its communities annually in the form of charity care and
other community benefit programs. Trinity Health employs about 119,000
colleagues, including 7,500 employed physicians and clinicians. For more
information, visit www.trinity-health.org. For more information, visit trinity-health.org. You can also follow Trinity Health on LinkedIn, Facebook or Twitter.
A new philosophy of
COVID-19 is circulating through the Republican Party and conservative
media. If you look closely, you might notice that it resembles an early
philosophy of COVID-19 that circulated through the Republican Party and
conservative media: If young people get this disease,it won’t be so bad—and it might even be good.
Scott Atlas, the new White House science adviser and Trump-whisperer, seems to be the ringleader of this emergent corona-stoicism.
A neuroradiologist and senior fellow at Stanford University’s
conservative Hoover Institution, Atlas is not an expert in epidemiology
or infectious diseases. As a Fox News regular, his relevant credentials
seem to be more televisual than scientific.
“It doesn’t matter if younger, healthier people get infected,” Atlas said in a July interview
with San Diego’s KUSI news station. “I don’t know how often that has to
be said. They have nearly zero risk of a problem from this … When
younger, healthier people get infected, that’s a good thing.”
The
reality is that, so far, COVID-19 has killed fewer children and
teenagers than seasonal flu in a normal year, according to data compiled
by the Centers for Disease Control and Prevention.
(COVID-19’s fatality rate is much higher than influenza, but school
closures and lockdowns have reduced teenage exposure to all sorts of
infectious diseases.) A 25-year-old who contracts this disease is
approximately 250 times less likely to die than an infected 85-year-old,
according to the most sophisticated estimates
of infection-fatality rates. For every 1,000 people infected with
COVID-19 under the age of 35, the average expected death count is less
than one.* These facts might give you the impression that, as Atlas said, “it doesn’t matter if younger, healthier people get infected.”
But it does. It really does. Here’s why.
Many young people
navigating this pandemic are asking themselves a two-part health
question: What are the odds that I get infected? And if I do get
infected, is that really a big deal?
Muchof myreporting
has focused on the first question. To summarize that work in a
sentence: People are at highest risk of infection in communities with a
sizable outbreak, when they spend long amounts of time in closed,
unventilated spaces where other people close by are talking or otherwise
emitting virus-laden globs of spit, and everything is worse when people
aren’t wearing masks. This advice is easy to give, because the best
practices hold across the board, for everybody.
“What’s the big
deal?” is a harder question, because the person-to-person outcomes of
this disease are so maddeningly variable. The most universal answer must
begin with the observation that death is not a synonym for risk.
COVID-19
presents an array of health challenges that are serious, if not
imminently fatal. The disease occasionally sends people’s immune system
into a frenzy, wreaking havoc on their internal organs. Several studies
of asymptomatic patients revealed that more than half of them had lung abnormalities. A March study published in the Journal of the American Heart Association found that 7 to 20 percent of sick patients showed heart damage associated with COVID-19.
As my colleague Ed Yong explained, many COVID-19 patients experience protracted illness. These “long-haulers”
suffer from a diabolical grab bag of symptoms, including chronic
fatigue, shortness of breath, unrelenting fevers, gastrointestinal
problems, lost sense of smell, hallucinations, short-term-memory loss,
bulging veins, bruising, gynecological problems, and an erratic
heartbeat. And according to the neuroscientist David Putrino, chronic
patients are typically young (the average age in his survey is 44),
female, and formerly healthy.
We don’t know how many long-haulers
are out there. But by combining the conclusion of several well-regarded
studies, we can arrive at a decent estimate.
For men in their 30s, like me, about 1.2 percent of COVID-19 infections result in hospitalization, according to a July study published in Science. Once the disease has progressed to this point, the risk of chronic illness soars. Research from Italy found that roughly nine in 10 hospitalized patients said they still had symptoms after two months. A British study reported a similar risk of long-term illness.
Now
the math: When you multiply the hospitalization rate for 30-something
men (about 1.2 percent) by the chronic-illness rate of hospitalized
patients (almost 90 percent), you get about 1 percent. That means a guy
my age has one-in-100 chance of developing a long-term illness after
contracting COVID-19. For context, the estimated infection-fatality rate for a 60-something is 0.7 percent, according to the same study in Science.
You
might be used to thinking of 30-somethings as safe and seniors as at
risk in this pandemic. But if a man in his 30s and a man in his 60s both
contract COVID-19, it is more likely that the 30-something will develop
a months-long illness than that the 60-something will die, according to
this research. (The calculation above doesn’t even include the
countless long-haulers who never went to the hospital.)
More
frightening than what we’re learning now is what we cannot yet know: the
truly long-term—as in, decades-long—implications of this disease for
the body. “We know that hepatitis C leads to liver cancer, we know that
human papillomavirus leads to cervical cancer, we know that HIV leads to
certain cancers,” Howard Forman, a health-policy professor at Yale, told James Hamblin and Katherine Wells of The Atlantic. “We have no idea whether having had this infection means that, 10 years from now, you have an elevated risk of lymphoma.”
Why would Scott Atlas,
the White House, or anybody for that matter dismiss the threat to young
people? One answer is that they want to convince Americans that if a
bunch of teens and 20-somethings get infected, the U.S. will move closer
to the ultimate goal of achieving “herd immunity.” Briefly, that means
the point at which a disease, like COVID-19, can no longer trigger an
epidemic outbreak, because enough of the population has already
developed immunity. Atlas has argued that, if herd immunity is an
inevitable destination, we should perhaps put our foot on the
accelerator.
But the case for herd immunity rests on two dubious
assumptions. The first is that the disease isn’t risky to the people it
doesn’t kill—which we know to be false.
“If
you’re signing up for herd immunity, you’re also signing up for a huge
number of hospitalizations, and a substantial fraction of those people
will be sick for months,” says Marm Kilpatrick, an infectious-disease
researcher at UC Santa Cruz. “Do the symptoms last three months? Six
months? Three years? Nobody knows, but I wouldn’t want my pandemic plan
to be Let’s have hundreds of thousands of young people with lifelong illnesses.
I wouldn’t want to tell 30-to-50-year-olds that we’ve signed them up
for a high risk of heart disease and chronic organ damage.”
The second dubious assumption is that it’s easy to distinguish between the high-risk group and the low-risk group.
“The
most simplistic way to protect the vulnerable is to divide the
population by age, but you can’t choose an arbitrary cutoff and say
‘Let’s protect everybody under age 65,’ because nothing magic happens at
age 65,” says Andrew Levin, an economist at Dartmouth. “The average
person who is 64.9 years old has the exact same health risks as somebody
who is 65. So it’s very difficult to divide populations into safe and
not-safe categories.”
Besides,
the U.S. is not, for the most part, spatially segregated by age.
Restaurants and stores serve old and young patrons, and there are tens
of millions of multigenerational households. Evidence that young and old
people mingle constantly can be seen in the recent COVID-19 death data:
A southern surge that started among young people spread to older
populations, who died in disproportionate numbers. “There is the
assumption that we can start cocooning the elderly, but we have no new
innovation here,” says Natalie Dean, an assistant biostatistics
professor at the University of Florida. “Are they saying we should try
harder to protect old people? What does ‘trying harder’ even look like,
compared to now? I just don’t understand the argument.”
Herd
immunity is an inoperable plan, teetering on a false assumption of
elderly-cocooning, which encourages young people to play craps with the
long-term health of their internal organs. The choice is yours. You can
listen to the scientists. Or you can roll the dice with your guts.

















/media/None/Derek_Thompson_grey/original.png)
{kind=link}